I woke up this morning thinking “Did I really end the last post by saying I had a ‘pink lace man-thong’?” and checked; yes I did say that. Then I wondered if there even is such an item. That’s why there is a thing called Google I guess. DO NOT CLICK ON THE FOLLOWING LINK if you are faint of heart … it is a link to Amazon (of course). THE LINK NOT TO CLICK because some things can not be unseen. Ever.
Anger is a tough issue. People tell me that I have a “right” to be angry now. Or that it is natural. I don’t think that I am particularly angry, at least not because of the cancer per se.
In 1989 I was lying on my bed watching TV and my then-wife came into the room. We had a “discussion” about something and I did get angry. I had the remote control in my hand and I threw it. Not at her, actually in a very different direction and it hit the ceiling near the wall across the room. That was just about 30 years ago, I remember it well. And I know the exact spot the remote hit.
 |
and zoomed in … |  |
These pictures were taken today. You may notice in the zoomed-in image on the right a faint outline around the marks … that is from painter’s tape placed over them because I will not allow them to be removed or covered. And the ceiling is actually white, so much for cell phone cameras.
The marks have lasted longer than the marriage did (and longer than the remote) but it was a good marriage (went on for 10 more years). That day was the last day I truly got angry. I look at the marks every so often to remind myself that anger is ugly, there are better ways.
I blogged about the cerberus II meeting of 16 days ago. Here is some other background that I don’t believe I have shared.
At the original cerberus meeting I asked if there was a chance that the surgeon would open me up, see that the cancer had spread and just close me up. He said:
No. Once you are on the table this tumor is coming out.
For whatever reason that made me feel ok. But, at a later date, when I was told I would get an MRI in August (the one from three weeks ago) I asked “why?” I was told that those results would tell us more about the tumor and if surgery was still a viable option. I don’t believe I shared that with anyone but it really fucked me up. This was before the start of chemo-radiation. I had the six weeks of chemo-radiation ahead of me, several weeks of “healing” and then that MRI to see if the cancer spread to the point of determining that surgery would not be an affective action. Every time that popped into my head was hell. I was very nervous about the CT and MRI scans and the results. I did not share my feelings with anyone, there was no point. I would not have felt better and they would most likely feel worse.
You can re-read the post about the cerberus II meeting but now you are aware that I was very tense about it. I was going to learn the result of the MRI and knew that there was a chance of hearing some very bad news. I arrived on time and they told me to sit and do nothing, the instructions for that day were bizarre and logistically impossible, etc. When they realized I was not happy, as I wrote, a nurse practitioner (NP) came in with someone else. It appeared that she was in some supervisory role but in my state I did not catch her name. Neither did Inanna who was sitting with me. The NP asked about some of the screwy things (my words) and photocopied the instructions I brought with me. She then asked me what else she could tell me.
I was angry. So much was screwed up and here I am, desperate to know results of my scans, it is past the time of the actual appointment to start, and I feel myself losing it. I glanced over at Inanna a couple of times and she was looking down. She has never seen me like this. Don’t get me wrong, I did not raise my voice, nor did I say anything inappropriate. Every filter in my brain was on DEFCON 1. Yet my anger was palpable, probably from 20 paces. I looked right in her eyes and all I could come up with as to what else she could tell me was the truth … “Did my cancer spread? Did the tumor shrink? Are we still having surgery?” I knew she would not answer any of these. She said she would go get the doctor.
I was livid. I was literally scared for my life. I knew NOTHING but I am sure she did. I know the doctors did. And there I sat.
As we waited I asked Inanna if I was out of line. She assured me I was not but that my anger was obvious.
It’s been thirty years since I was in that state. I wanted to throw something. I wanted to rip into the staff. I wanted to know how close I was to dying. All I wanted to know was what they knew.
A couple of days later I wanted to reach out to that nurse practitioner, but I did not know her name or even if that was really her position. I would have apologized or explained, I felt bad that I was in that state. Again, I was sure that I did nothing “wrong” yet I hoped to connect.
It didn’t happen. Until two days ago.

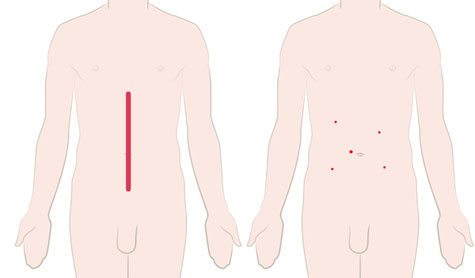
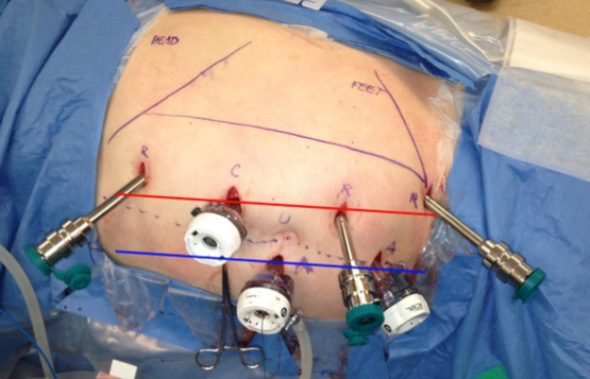
 “Open and laparoscopic abdominal incisions after urgent total abdominal colectomy for CUC. Left panel: laparotomy with staples; right panel: laparoscopic subtotal colectomy with one 12-cm port site hidden in the diverting stoma, three 5-mm suprapubic, and 1 left lower quadrant ports are imperceptible. Left panel courtesy of Holubar; Right panel courtesy of Dozois, May Clinic, Rochester.” From
“Open and laparoscopic abdominal incisions after urgent total abdominal colectomy for CUC. Left panel: laparotomy with staples; right panel: laparoscopic subtotal colectomy with one 12-cm port site hidden in the diverting stoma, three 5-mm suprapubic, and 1 left lower quadrant ports are imperceptible. Left panel courtesy of Holubar; Right panel courtesy of Dozois, May Clinic, Rochester.” From 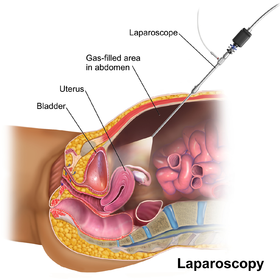 There are a number of advantages to the patient with laparoscopic surgery versus the more common, open procedure. Pain and hemorrhaging are reduced due to smaller incisions and recovery times are shorter. The key element in laparoscopic surgery is the use of a laparoscope, a long fiber optic cable system which allows viewing of the affected area by snaking the cable from a more distant, but more easily accessible location.
There are a number of advantages to the patient with laparoscopic surgery versus the more common, open procedure. Pain and hemorrhaging are reduced due to smaller incisions and recovery times are shorter. The key element in laparoscopic surgery is the use of a laparoscope, a long fiber optic cable system which allows viewing of the affected area by snaking the cable from a more distant, but more easily accessible location.