Many of you know me as SingleDad from my blog Disabled Daughter. For six years I blogged about my life as a single father with two severely disabled children. Pearlsky lived with me; David was in a residential school. I stopped blogging when life became difficult for reasons known by the followers of that blog. But here I am. No longer a single dad, and quickly becoming disabled myself.
I was diagnosed with stage 3 colorectal cancer on April 24, 2018. There have already been so many events that I want to blog about. Events with me, with Pearlsky, with Inanna, and more.
If you want to follow this blog, sign up on the right. The list is separate from SingleDad’s.
And by the way, cancer sucks.

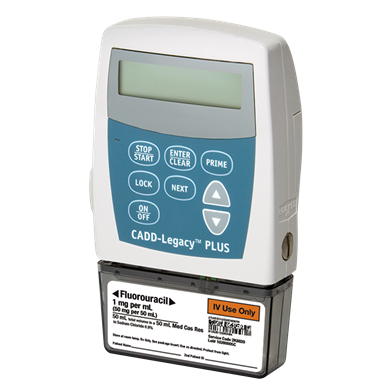
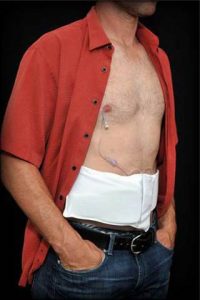 I will sleep with it in a PoppyPocket on my stomach, I do not sleep on my stomach, it should work. I have ordered a Spongebob patch for my black fanny pack that I will be using during the day. Why not?
I will sleep with it in a PoppyPocket on my stomach, I do not sleep on my stomach, it should work. I have ordered a Spongebob patch for my black fanny pack that I will be using during the day. Why not?