[Trigger alert: sarcasm ahead]
Seeing that I am a man’s man, a manly man, a man’s kind of man, I am very nonchalant and totally unconcerned about tomorrow morning’s CAT scan followed by an MRI.
I have no issues about taking an overnight laxative tonight. A self inflicted enema tomorrow morning, no problem! Getting to the hospital an hour early to drink a quart or two of not great tasting something, I laugh in it’s face! Lying in a CAT scan for about 20 minutes, then the MRI …
Before entering the room for the exam an IV catheter will be placed to allow access during the exam for the use of an IV contrast agent called gadolinium. The IV contrast agent will be injected toward the end of the exam and will increase the information obtained. If you have any questions about the use of contrast agents for your exam please contact the MRI department.
Once inside the exam room, a Radiologist or Nurse Practitioner will place a small plastic tube called a catheter into your rectum. A liquid barium contrast agent will then be injected through the catheter and into your rectum and will remain there until the exam is completed.
I am so fucking excited I could just shit.
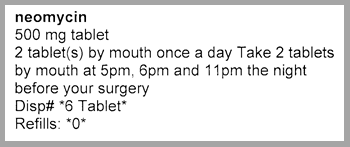
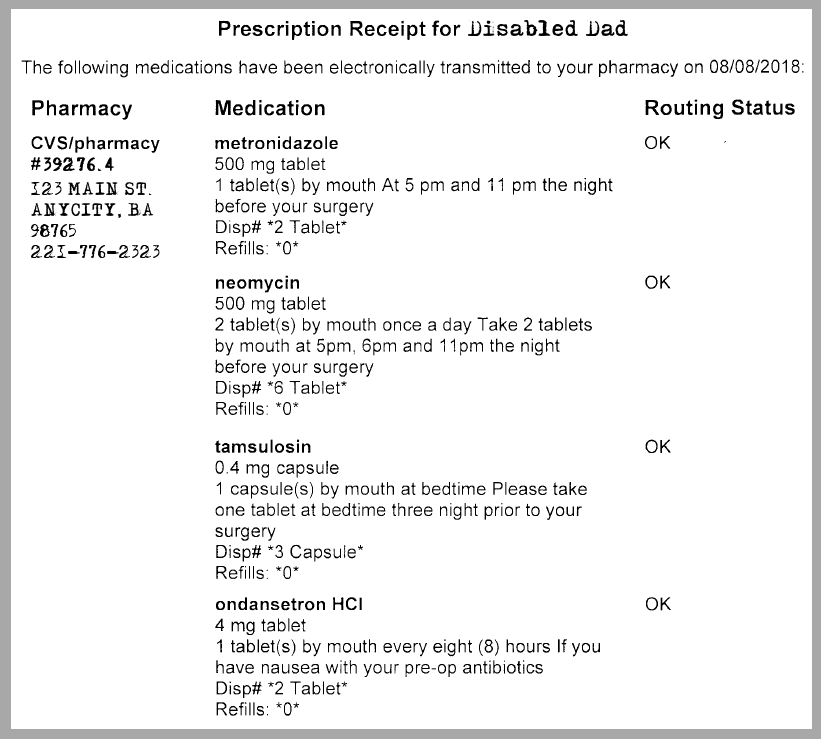
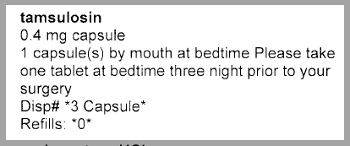
Why does one have anxiety about a medical test? The test itself will not change anything about my body or health (for all intents and purposes). The fear of the test itself may be from not knowing what the test entails. In this case, I know what it entails; taking a laxative, giving myself an enema, getting an IV in my arm, getting a shot (somewhere), having a catheter shoved up my ass, receiving a bolus of barium via said catheter, and then lying in a tube so small I can’t move my arms for close to an hour. Of course there is no anxiety, I know exactly what will happen.
Would there be fear of the result which some people will know immediately yet I need to wait two days? That gives two days of waiting which always just sucks. But again, that is not too anxiety producing. And whatever my status is tomorrow during the test is what my status is as I write this. The difference is not in my tumor, it is in my knowing.
So what’s the anxiety thing, which of course a man like me does not have?
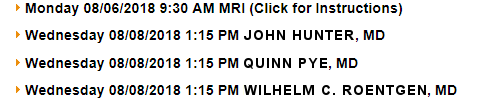
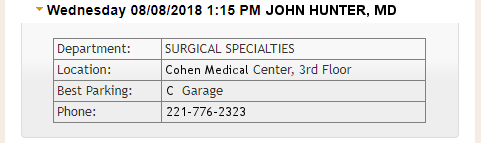
The CAT scan and the MRI are tomorrow. The flexible sigmoidoscopy exam is Wednesday. The results of all three follow an hour later during the cerberus II meeting. No anxiety there.
What we will learn:
- Exact location of the tumor
- The current size of the tumor
- Has the cancer spread to the lungs (easier to write “the” than “my”)
- Has the cancer spread to the liver
- Is surgery even worth doing?
- Is it true that there is no tumor, but we found Judge Crater?
By the way, Judge Crater disappeared the actual day my father was born, and both events were about 3 miles apart. Hmmmm … and tomorrow, the day of scans, is both my day’s birthday and the anniversary of Judge Crater disappearing. Coincidence? I think not!
Ok, so now that we have totally reasoned away the thought of anxiety or fear we can move on with our life. Oh, wait, don’t know if we can. I don’t know if I can move on with life, but I may know on Wednesday, two days after others know.
I hate this shit. Where’s my medical marijuana …