My daughter, Pearlsky, is severely disabled. She is totally dependent on others, non-mobile, non-verbal, has no known form of communication. For twenty-five years I have strived to make her quality of life, from HER point of view, to be as good as possible. At the same time I have a prayer, I pray that she does not know she is disabled to the degree she is. Because there is no communication, we don’t know what she knows.
I am quickly going from being a caregiver to a care taker. My mind is not affected at all, but my body is being beat up. I am starting to struggle in caring for Pearlsky, and may reach a point where caring for my self is a challenge. Advocacy work, and working with the district is not an issue, I am doing much by phone and informal meetings at good times of day for me. It is tough watching myself go from helping others to needing help. I am officially a person with a disability.
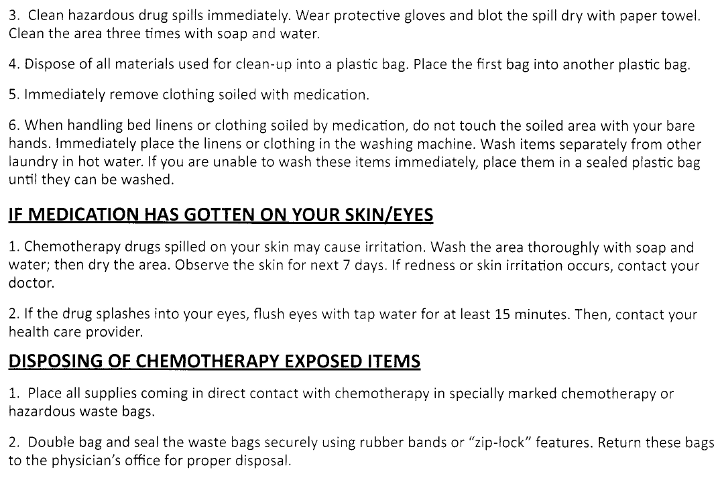
Many of us become disabled; most often because of growing older, an accident, war injury, and the like. I come by my disabilities in a different manner; I choose to lie on a radiation table daily. I choose to wear a pump sending poison throughout my body 24/7. I also know that there are two possible outcomes in the months ahead, and either way the disability will end.
It must be getting to me; I can’t even play the cancer card effectively …