
What follows will appear to be a non sequitur but it ain’t (you can skip this first part if you want) …
My dad was a great guy. A lifeguard who, at 18, spotted my 15 year-old mother, fell in love and was with her for 62 years (and in some ways beyond); a college football player (proclaimed “fleet-footed” by the city’s newspaper); earned a degree in physical education; a fighter-bomber pilot and captain in the Strategic Air Command, and a long time drug pusher. Well, let me explain that last one. Dad joined Stuart Pharmaceuticals around the time I was born and he traveled around interfacing with doctors (a “detail man” now known as “pharmaceutical sales representatives,” or simply “drug reps”). Stuart was a division of Atlas Chemical Industries which in turn was bought by ICI Americas Inc. (1971), which then partially de-merged into a new company, Zeneca (1992). That did not last long; Zeneca the merged with Astra AB to form AstraZeneca (1999). Dad stayed along for the ride, starting as a drug rep, ending up in charge of all domestic drug sales by his retirement. The eight-year mark of his ultimate retirement is coming up in November, I still miss him very much.

Dad was the first person to ever sell the antacid Mylanta. During the early 1960’s Dad was working a pharmaceutical convention. It was a Sunday, the last day of the trade show; Mylanta was to be introduced as a product the next day. Dad called his boss and got permission to talk about it that last day, and he did. Personally I think that’s kind of cool. It is not so great knowing that people’s ulcers, the primary drive for Mylanta sales, are what paid for my college, but it did work out well for me.
During his career, Dad was involved with many products including but not limited to Mylanta, Propofol (aka Diprivan a very common anesthetic), Tamoxifen (aka Nolvadex – breast cancer treatment), and Hibiclens (skin cleanser and antiseptic). It is the last item, Hibiclens that makes all of this pertinent and not a non sequitur. Really.
Hospitals are doing all they can to prevent infections, especially when surgery is involved. One way to do this is to ensure as sterile a surgical field as possible. Many are asking patients to wash with Hibiclens, or a generic version, the night before surgery and the morning of. It is easy enough and is proven to be effective for at least 24 hours.
During college I found that many deodorants caused me rashes. I tried an experiment and found that using Hibiclens twice a week (I did have access to the occasional sample bottle) would actually be most effective. I had the sterile-est underarms on campus. I have used it over the years and it works extraordinarily well.
During the preparation talk, the nurse mentioned showering with Hibiclens the night before, and the morning of surgery. She indicated that there was a bottle in the blue plastic bag she brought with her. She then went on to explain how to use it …
Use this to wash between your neck and your hips only. Do not wash your head, groin or limbs with it. Shower with it the night before, and the morning of your surgery.
I asked specifically if I could use it on my underarms and upper arms and she responded …
No, that is not where your surgery is. Only from your neck to your hips, not your limbs.
I knew better than to argue or continue this conversation. It is, actually, important to not get it in your eyes or your ears, but that is about it.
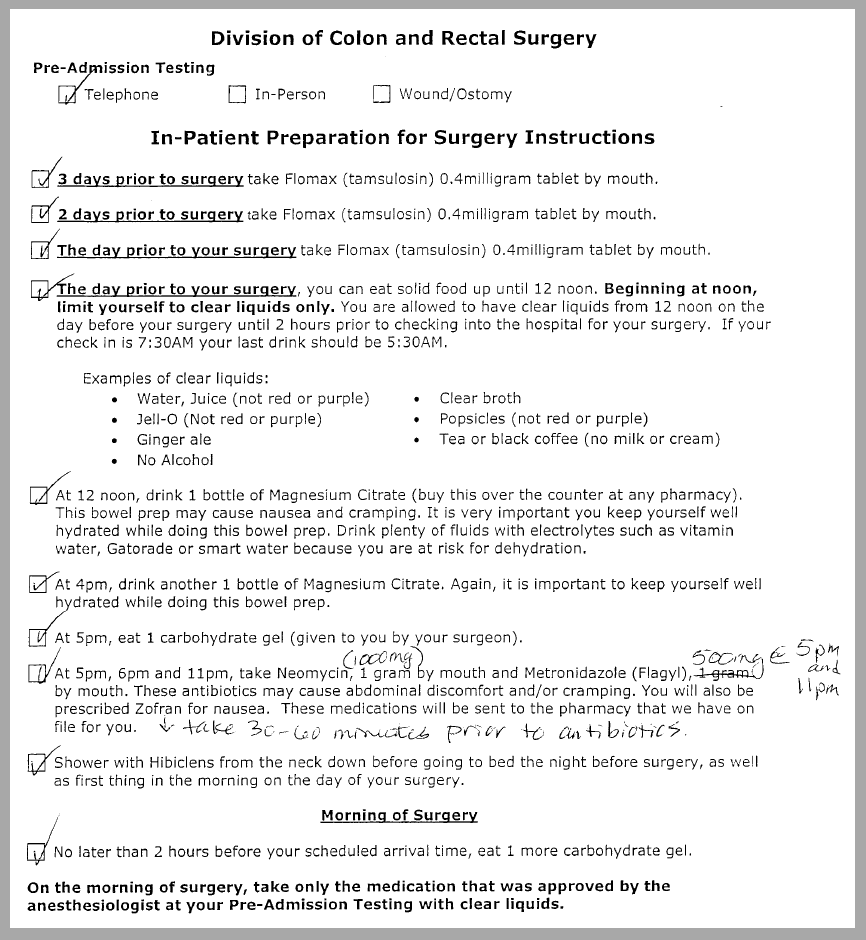
Luckily this is all it says on my (her?) checklist:

Good thing I was listening carefully since the written information does not have the dire limb warnings.
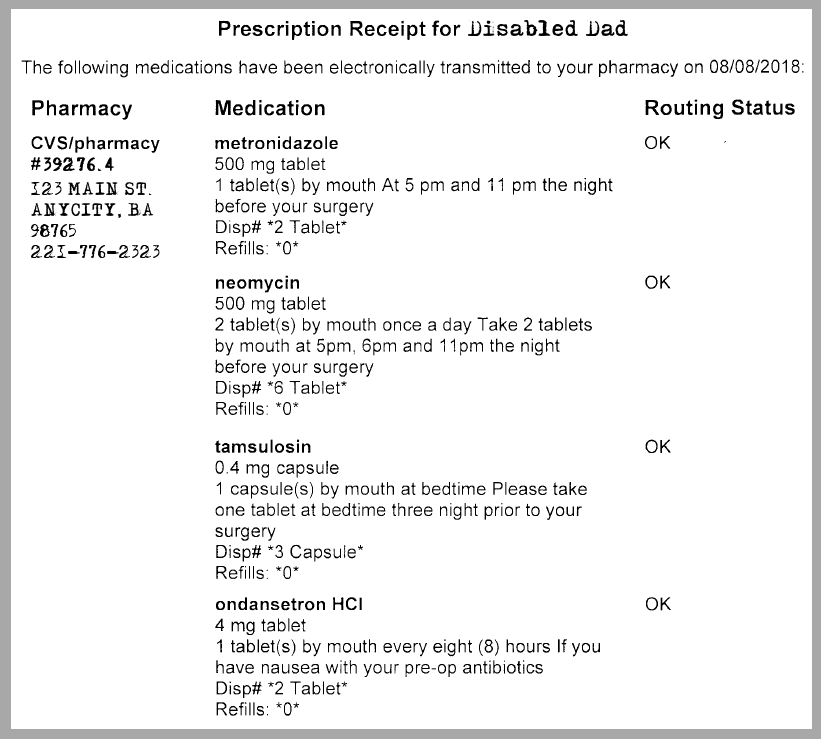
At home I look in the blue bag she gave us and there is a piece of paper wrapped around the bottle of surgical soap. Here is what it says:
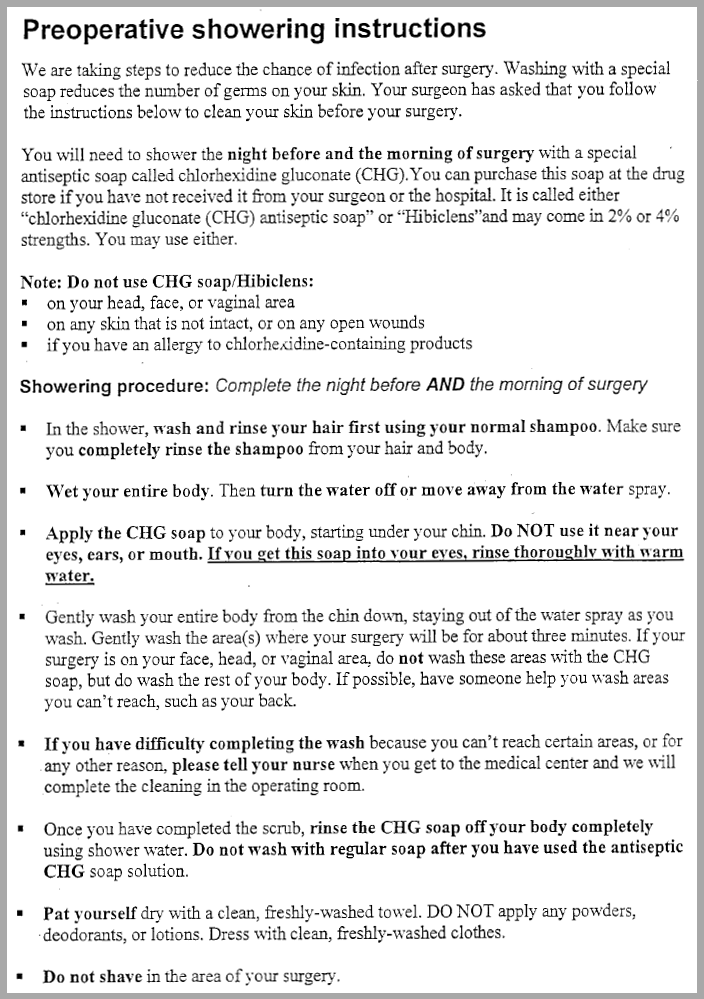
Now we have some real instructions we can work with.
Ok, I got this. Keep it away from open wounds. Don’t use if you are allergic to it, and do not use on your head, face or vaginal area. The head and face warnings are because of the danger of getting it in your eyes or ears (which is a serious concern with the primary ingredient CHG). The importance of keeping it away from your vaginal area is because Hibiclens will stain the sheets and the closest thing to “my” vaginal area is usually still in bed when I shower. (Using chlorine bleach on fabric that has a Hibiclens stain will cause it to turn brown and be permanent, just saying.)

Yet another warning about eyes, ears, and they add your mouth (note, the active incredient, CHG, is also in Peridex, the dental mouthwash). It is highlighted that if you get it in your eyes you should rinse thoroughly with warm water. If you get it in your ears, mouth or vaginal area I guess you are just shit out of luck and there is nothing to do.
And finally we have:
Right. Got it. “Gently wash your entire body … wash the rest of your body …” What about my limbs? Are they included in “entire body” or are they part of my out-of-body experience?
“What does the manufacturer say?” Glad you asked:
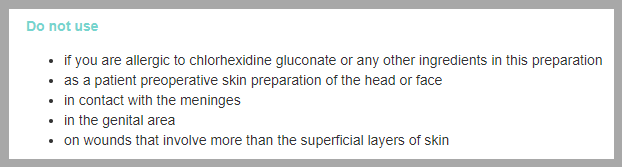
The “meninges” is the stuff that surrounds your brain and spinal cord, minimal chance of getting the soap in contact with it, but no one warns you for that! “If your brain or spinal cord are exposed, do not wash them with this product.”
To get serious, yes, I get it. This is just about soap and washing. It is very important for infection control yet a simple thing to do. What I find incredibly maddening is the inconsistency between written directions and oral directions, and even between two pieces of paper with what should be the same directions. The previous post is about the medication directions and how they are non-sensical and contradictory. We see the issue here as well. I do not understand this. Why would the nurse specifically tell me I cannot wash my limbs and underarms when in fact of course I can? Again, what or whose instructions do I follow?

No comments yet on this ↑ post, add yours (or read theirs)