
Two weeks until surgery and yes, I am getting nervous. I am preparing by preparing and learning. In this post there will be some pictures that are hidden and you can choose to look at them. No, not pictures of me. At least not yet. They will be behind a click me thing that just makes them appear, it does not take you to a new page. Here is a test to show you a secret message:
Click here for the secret message
I have colon cancer. Cancer sucks.
I will also do that with more technical information. People have asked all sorts of questions about the protocol and surgery and I will answer some today, in this post.
The goal of the chemoradiation was primarily to shrink the tumor and kill cancer cells that were in the surrounding tissue. It has been found that for certain tumors doing chemotherapy along with radiation makes both of them more effective. I had this for six weeks.
To read a bit more technical information on it, click here
Chemoradiation therapy in the management of gastrointestinal malignancies.
McRee AJ1, Cowherd S, Wang AZ, Goldberg RM.
Abstract
Concurrent administration of chemotherapy and radiotherapy has been increasingly used in cancer treatment, leading to improvements in survival as well as quality of life. Currently, it is a feasible preference, often regarded as the standard therapeutic option, for many locally confined solid tumors, including anal, bladder, cervical, esophageal, gastric, head and neck, lung, pancreatic and rectal cancers. In patients with these tumors, combined modality therapy improves local tumor control and survival while, in some instances, obviating the need for surgical removal of the organ of origin. The scientific rationale for the use of chemoradiation derives from the preclinical and clinical observations of synergistic interactions between radiotherapy and chemotherapy. When chemotherapy and radiotherapy are administered together, the chemotherapeutic agents can sensitize the cancer cells to the effects of ionizing radiation, leading to increased tumor-killing effects within the radiotherapy field. This, in turn, can improve local control of the primary tumor and, in some cancers, render surgical resection unnecessary. In other cases, patients with tumors that were initially considered unresectable are able to undergo curative interventions after completing chemoradiation. The chemotherapy component can address any potential micrometastatic disease that, without therapy, leads to an increased risk of distant recurrence. A large body of evidence exists that supports the use of chemoradiotherapy in gastrointestinal cancers. In fact, one of the first tumor types in which the superior efficacy of chemoradiation was described was anal cancer. Since then, chemoradiotherapy has been explored in other gastrointestinal malignancies with superior outcomes when compared with either radiation or chemotherapy alone. This article aims to recapitulate the clinical evidence supporting the use of chemoradiotherapy in a variety of gastrointestinal tumor types.
From here.
Then there is the question as to why I am waiting for surgery? In the beginning (sounds so biblical) they tried surgery after chemoradiation but found that it was not working too well. Recently radiated tissue is very difficult to work with and the surgeons found that some tissue was just falling apart, suturing was difficult, etc. So they waited two weeks. That did not work out so well and they tried waiting four weeks. By the time they waited 12 weeks they determined that was too long. The wait is typically 8-10 weeks. During this time the chemo and radiation still have effects on the tumor and the body.
I have had side effects start several weeks after the chemoradiation ended. Dry skin primarily on my palms started about 2 or 3 weeks after therapy ended and my pubic hair actually started to thin about 4 weeks after. At this point I believe all side effects are done.
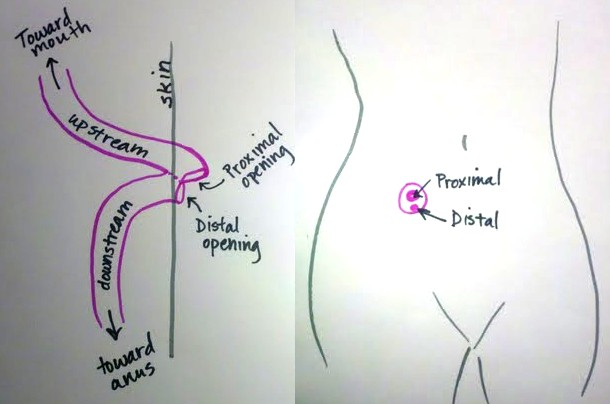
Let’s do a thirty second review from high school biology … here is something most of us have in common:
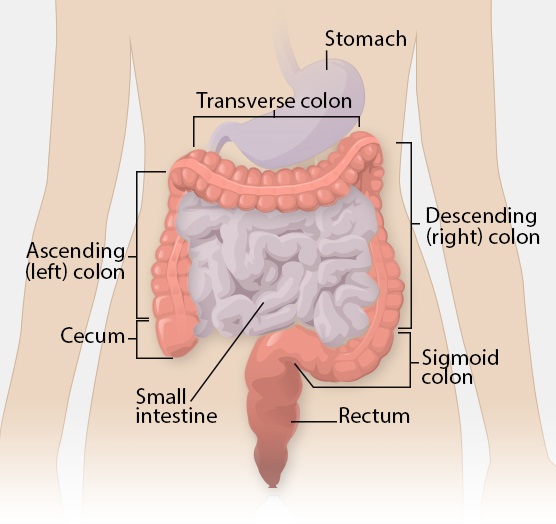
And of course the rectum exits at one’s butt.
I found a great resource with information about my upcoming surgery from the University of Tennessee Medical Center. I will be sharing parts of it in this post.
This picture is really freaky in that the black dot is in the original picture in that document. Why is that freaky? It is exactly where my cancer is … hmmmm … copyright infringement?
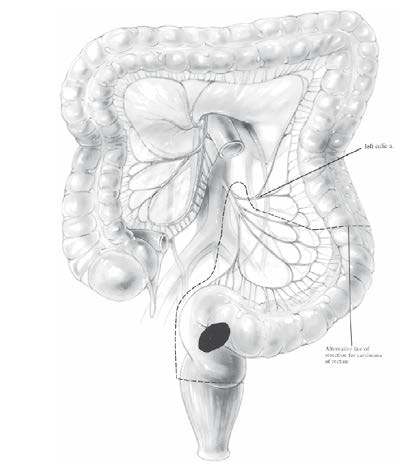
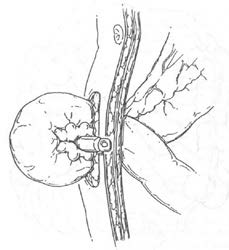
The dashed line shows what will be removed. There is enough of the rectum remaining to still be usable! The stringy things you see that will be removed are lymph nodes and blood vessels. Once this is removed, the new end of the descending colon will be attached to the remaining part of the rectum (since there is room for the surgeon’s stapler).
Click here for a better, more realistic picture
I added the black dot and the grey oval; that oval encloses what needs to be removed. 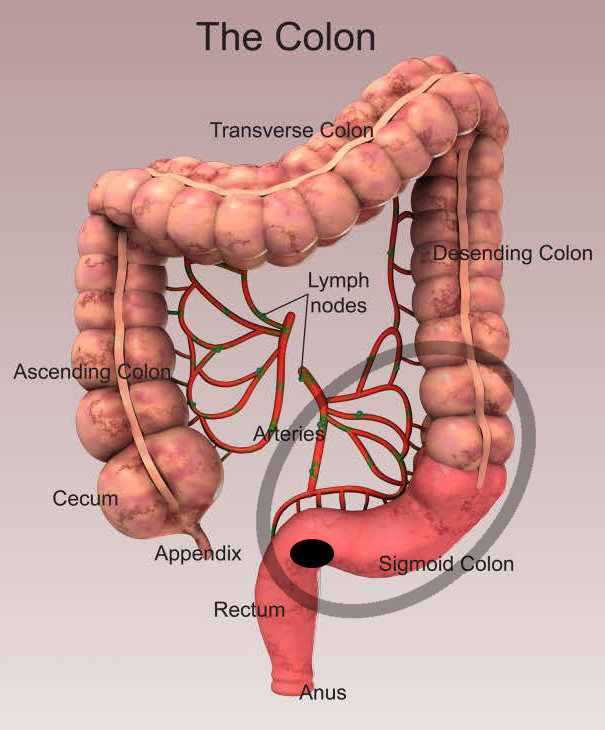
Once the bad shit is removed and the remaining colon is connected to the remaining rectum the question becomes, how does the connection heal? It cannot be all that helpful for me to be sending my poop, feces, shit, etc. past the new connection all the time. So that area is bypassed.
The bypass happens in the small intestine. Before the contents of the small intestine can reach the large intestine (colon) they are diverted out of the body. The large intestine does many things (and I am sure not all are known) but one primary function is to absorb water and salts. When the small intestine is diverted out of the body, what comes out is much more watery and unformed that what we are used to leaving our body. This can cause dehydration since the colon is not absorbing this water before it is lost.
This diversion, for me, will be temporary. The small intestine is diverted out the wall of my abdomen and that creates a stoma. This happens in the part of the small intestine known as the ileum, hence I will have an ileostomy.
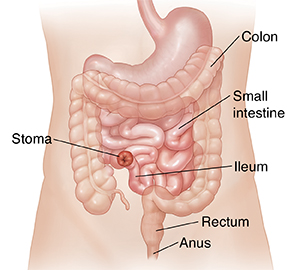
This is how it is done for a loop ileostomy:
Click here for more information on stomas (and pictures)
Two drawings of the surgery:
 |
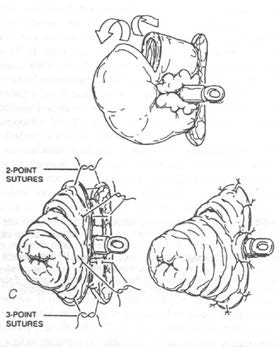 |
When you look at the actual stoma it is bright red/pink and moist because you are actually looking at the inside lining of the small intestine. And, yes, that is called the lumen!
Click for a picture of an actual stoma
 And no, he did not pull a quarter out of his stoma … that is to show the size!
And no, he did not pull a quarter out of his stoma … that is to show the size!
Depending on how my innerds are healing, I will have the stoma removed (all put back together) after about five weeks or five months. They don’t do that surgery during chemo which will start about five weeks after surgery.
And all of this will be complete, B”H, two weeks from right now.
Next post will talk about much more fun stuff, robotic surgery!

My sweet Grandma Sally had a permanent ilieostomy.
She adjusted so well that her surgeon would call her to come and counsel and comfort some of his pre-surgical patients. ❤️
Wishing you all the best and Shana Tova!