Which brings us to a favorite word of mine, einfühlungsvermögen (it’s pronounced just like it sounds) or Einfühlung for short. Loosely translated, it means to be able to understand someone else’s feelings. But until 1909, there was no real alternative to einfühlungsvermögen in English. The British psychologist, Edward B. Titchener, thought einfühlungsvermögen represented a powerful concept, but realized it would never catch on if it couldn’t be pronounced. So he invented a new word, easier to pronounce and similar to the existing English word sympathy. He created the term empathy.
Empathy is distinguished from sympathy in that it is not just about the ability to feel for someone else. Empathy involves being able to take someone else’s perspective. Which brings us back to our working definition for achieving relevance:
Empathy is the ability to stand in someone else’s shoes.
I started as a [Boston University’s overall youngest tenure track] professor of engineering design and progressed into having my own engineering company designing computer type stuff (jtag in-circuit emulators, if you must know). For analogy sake, let’s say I designed microwave ovens. I would do the engineering design, user interface, etc. and see that it gets to market. After about four months, a new revision or version of it would come out. Why? What is special about four months? Why were some new features added and some fixed?
- Customer feedback / complaints?
- Catching up to a competitor?
- My spouse left town?
The actual answer is “3,” my spouse (or partner or roommate or chef) left town and I had to use the microwave myself. Whenever I used my own product for the same reasons as, or in the manner of my customer, or rather, the device’s end-user, I found all the problems and missing features. In other words, I had to be the customer / end-user, not the designer, to fully understand that I needed a “popcorn” preset.
Unless I walked in the user’s shoes, the design was not all it could be. Or needed to be.
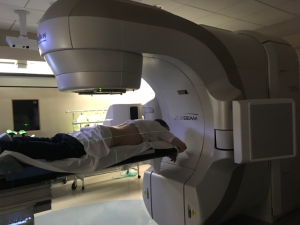
I have been in Truebeam for the last 24 weekdays. As you know at this point, I get up on that table, pull down my pants and manly panties, and lie on a white sheet. The machine projects three-green cross hairs. Two radiation therapists, one on each side of me, grab the sheet and coordinate pulls and tugs to move me into the precise position (i.e., each cross hair on a particular blue-dot tattoo).
Each set-up costs 3–5 million dollars. The machine, the table, the room with its 14 inch thick walls, the computer systems, etc. Oh, and the white sheet for tugging.
Give me $500 and a month and I will make it controlled with two joysticks. Better yet, for $1500 I will make it all automatic. Really. Design and prototype. Better yet, a barter … I will give you a working prototype, you get this fucking tumor out of my ass.
My point? Truebeam designers have never been treated for rectal cancer with their device. Or they have never watched what happens when I get onto it. My experience in their machine is complete foreign to them; they only have their assumptions.
There are many sympathetic people in my big-city hospital (except for two who can use some major re-training). I respect these people and I guess I appreciate their sympathy, but if I thought about that more, maybe not so much.
Empathy? Nope. Nada. Crickets. Othing-nay.
Handing me an enema and pointing me to a dirty bathroom floor to take it on shows either a total lack of empathy or shows that one just does not care.
To get the tattoo targets I had to lie on a different machine, in a different building, with several techs around. And a young intern. I had little idea what was going to happen, I was told I would not feel anything. At one point I felt something strange on my skin. I had to ask what was happening and someone said they were “drawing” on me. Why not preface it with the truth:
I need to write on your skin a bit. It is not permanent but will take you about a week of scrubbing your skin raw to remove it. Ok?
I don’t know about you, but I honestly found that someone writing on me without my knowledge to be extremely invasive and bothersome. A simple “I need to highlight this spot with a pen” would work. Is it ok with you if your doctor needs to draw on your body for some reason and just does it? Your dentist? Gynecologist?
You don’t have to have empathy, nor sympathy for that matter. I have cancer and will let you do what you need to in the hopes that I survive. To a large degree your actions determine how emotionally difficult, how logistically difficult, my fight will be along the way. It’s the smallest thing that sometimes make the biggest difference.
What if this was you?