I had two appointments today, the wound/ostomy nurse and the pre-admission testing.
I decided that I was not going to ask questions if I knew I could get the answer elsewhere. I was just going to smile no matter what. I am so beat down by this place, it is a survival strategy.
The wound/ostomy nurse appointment was for 10. I arrived at 9:45 in case I had to squeeze in an enema … you never know. I checked in, sat down and waited. At 10:15 I was craving coffee so I figured I would see how much of a delay there was. I walked up to the desk and simply said:
Do you know what time I may be called in?
The woman responded:
She may be running late.
May? She may be running late?
According to that clock on the wall it is determined that in fact she is running late, that’s not the issue. Do you know when I may be called in?
She made a phone call and no, I did not have time to get coffee.
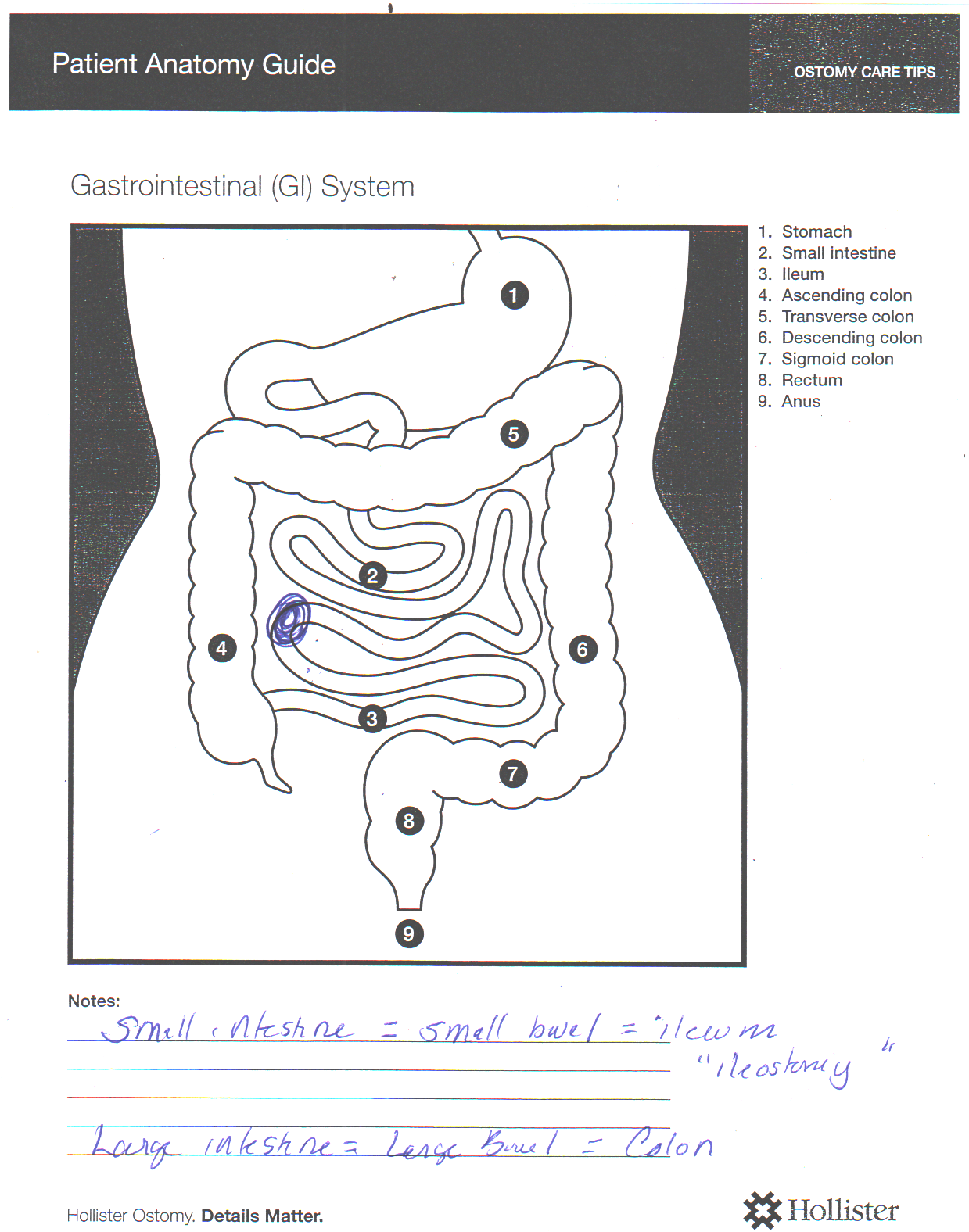
A very nice woman comes to get me, she is the nurse and apologizes for the delay. I smile and say “no problem.” I take her card and after her name it says “RN, BSN, CWOCN, Certified Wound, Ostomy and Continence Nurse” and I am a bit impressed even though I have no idea what some of that means.
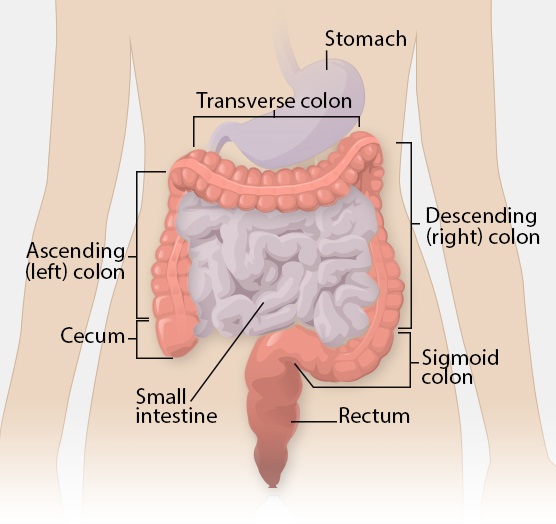
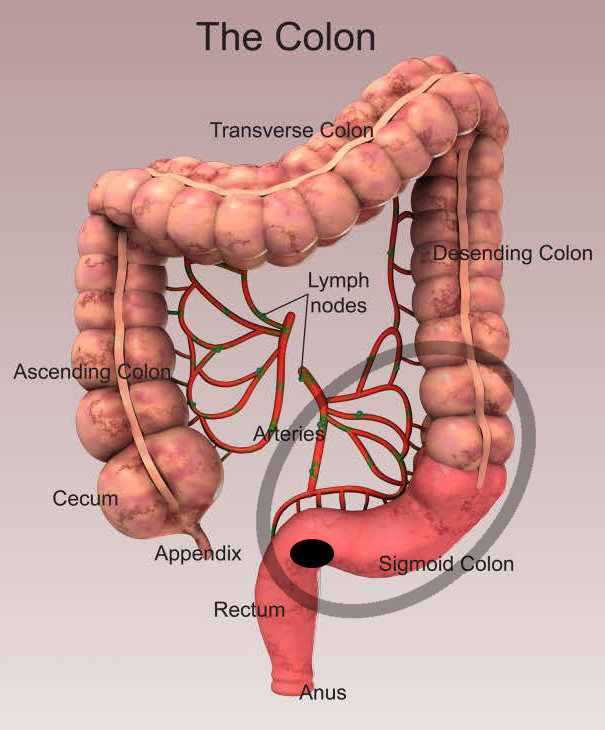
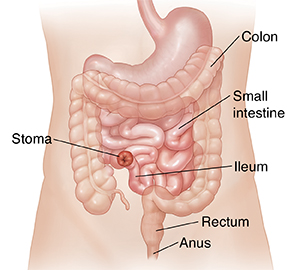
She started by telling me that she will talk to me as she talks to everyone. Yeah, I got that message loud and clear. That’s fine, I will smile and listen. She then taught me that the small intestine is sometimes called the small bowel, and she wrote this down for me. Then she wrote down that the large intestine is the same as the large bowel and that is also called the colon. She literally wrote this down for me.
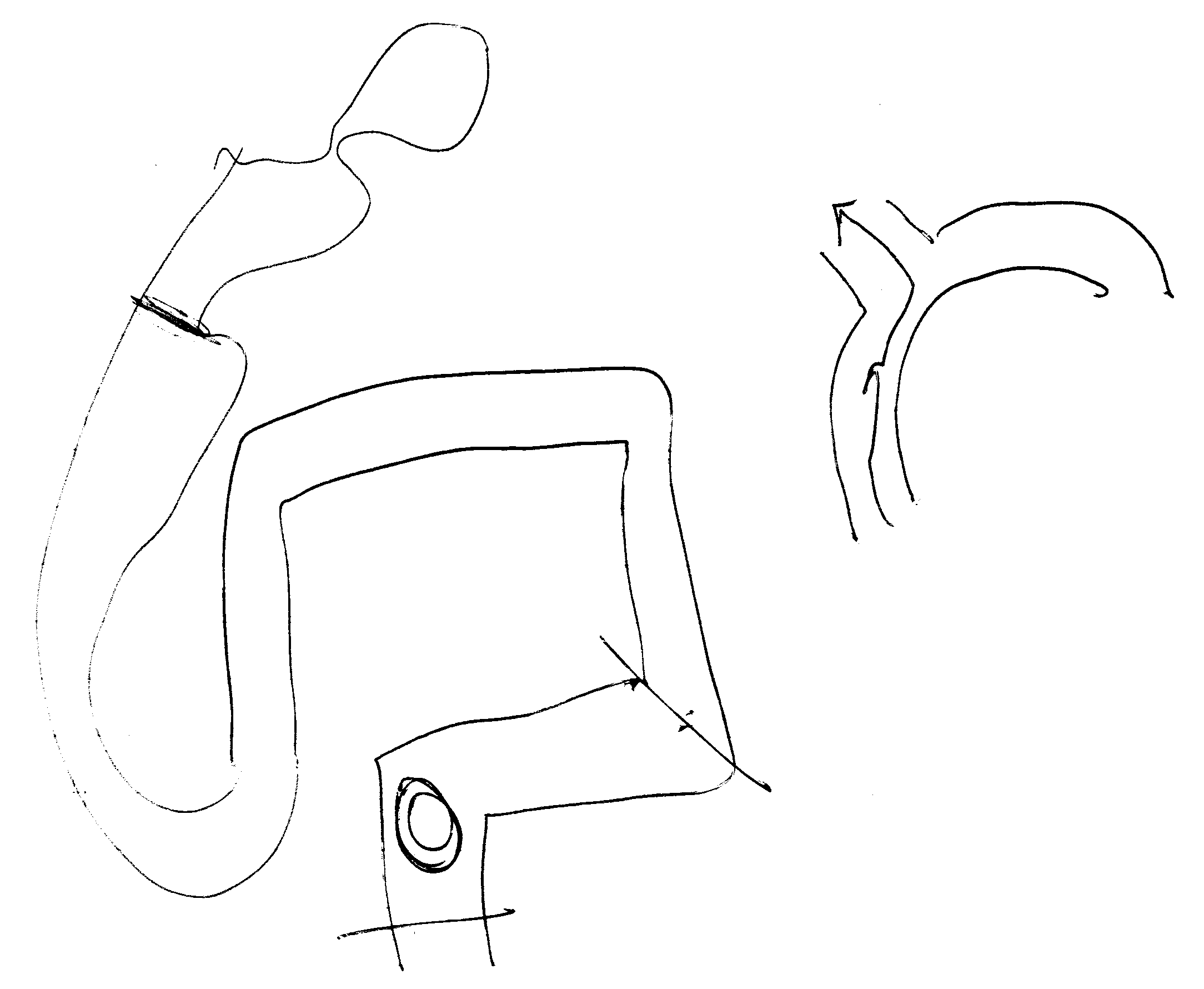
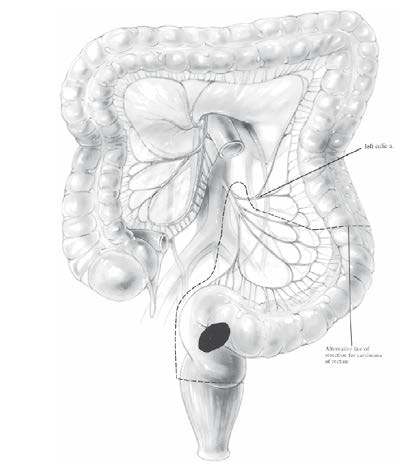
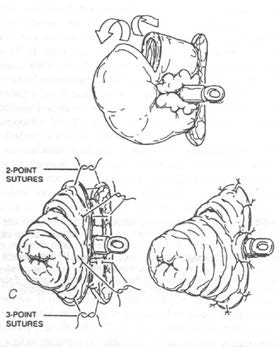
She had a great picture of what the surgery will do, but that is the only thing she showed me that was not part of my packet to go home. I really don’t understand why they would leave that out, but I did ask (yes, breaking my own rule) if I could have a photocopy of the paper she put away in her drawer. She did make a copy.
During her talk she used vocabulary all over the map. She taught me the words intestine and bowel yet used the word lumen three times and even in context I have no fucking idea what lumen means. I thought I knew what edema is, but in its context I am not sure. No, I did not ask, she knew her presentation, and since she is using low-level vocabulary (what ‘I will talk to you as I talk to everyone’ is code for) I am not going to show my stupidity. I am sure every patient in the clinic is familiar with their lumen. The whole thing started to make me bilious. And yes, that is another word she used and no, I had no fucking idea what bilious meant. Every time she said a word I did not know, I wrote it down.
Why they just don’t make a 15 minute video that explains all this that they can very carefully vet so it is understandable is beyond me. They can show it with the nurse sitting right there and all this goes away. But I digress … a bad habit of mine.
She had a show and tell with bags and stuff, I will share that in my next post.
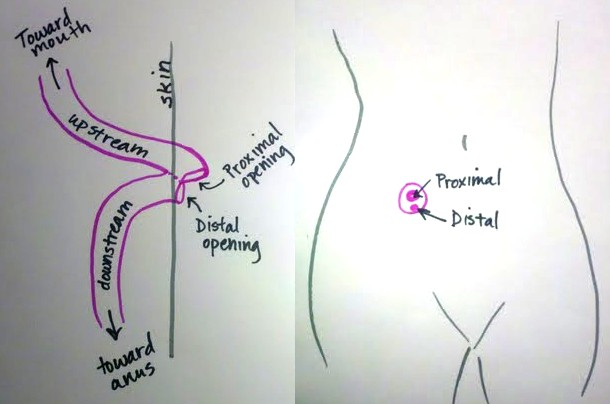
She then checked out my belly … mentioning that it was very nice (medically) and noticing that I am somewhat hairy so I should use my electric razor in the area of the ostomy. Ok, no problem. She looked at me sitting, lying down on my back and right side, saw how high (or low) I wear my pants and now “X” marks the spot. Pictures of my very nice belly and “X” coming soon.
I left her at 11:10 and I had a 5-minute appointment with pre-admission testing at noon. Remember, this is the one I was told would be done over the phone, but nooooo …
I went to the cafeteria on my way, had a portobello stew thing over whole wheat colored pasta for $4.95. Actually it was pretty good. Then onto pre-admission testing.
The appointment lasted 7-minutes. It consisted of 6-minutes of questions that could have been asked over the phone and the nurse looking in my throat. I will need to be intubated during surgery (breathing tube in my throat) and she needed to see if I have an appropriate throat, sans edema of the lumen.
Then I went home, curled in a fetal position, and cried.










 What better cover to use when sitting around just shooting the shit with friends?
What better cover to use when sitting around just shooting the shit with friends?

 And no, he did not pull a quarter out of his stoma … that is to show the size!
And no, he did not pull a quarter out of his stoma … that is to show the size!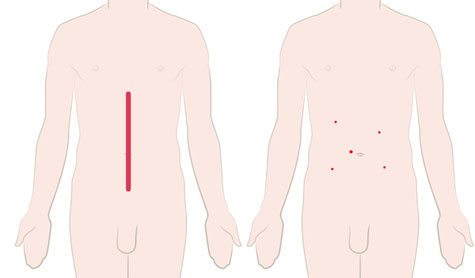
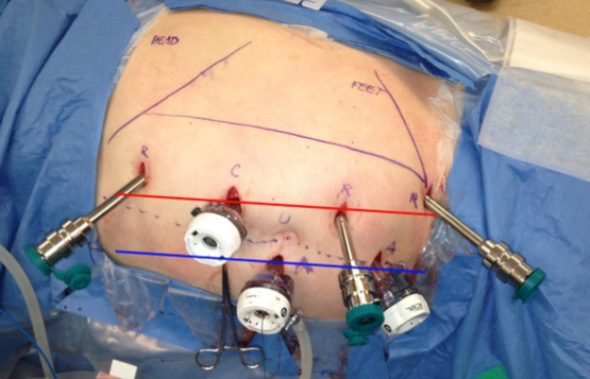
 “Open and laparoscopic abdominal incisions after urgent total abdominal colectomy for CUC. Left panel: laparotomy with staples; right panel: laparoscopic subtotal colectomy with one 12-cm port site hidden in the diverting stoma, three 5-mm suprapubic, and 1 left lower quadrant ports are imperceptible. Left panel courtesy of Holubar; Right panel courtesy of Dozois, May Clinic, Rochester.” From
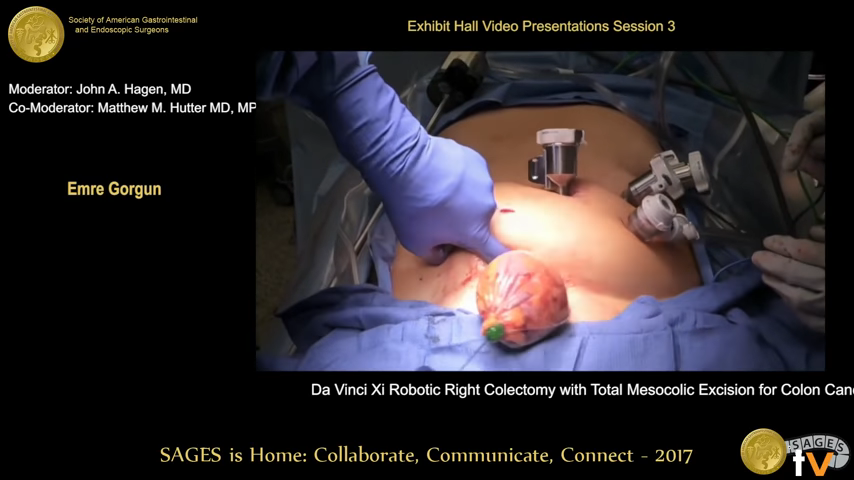
“Open and laparoscopic abdominal incisions after urgent total abdominal colectomy for CUC. Left panel: laparotomy with staples; right panel: laparoscopic subtotal colectomy with one 12-cm port site hidden in the diverting stoma, three 5-mm suprapubic, and 1 left lower quadrant ports are imperceptible. Left panel courtesy of Holubar; Right panel courtesy of Dozois, May Clinic, Rochester.” From 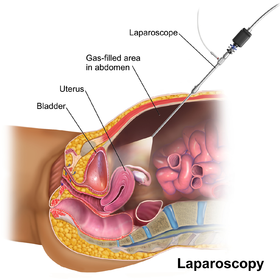 There are a number of advantages to the patient with laparoscopic surgery versus the more common, open procedure. Pain and hemorrhaging are reduced due to smaller incisions and recovery times are shorter. The key element in laparoscopic surgery is the use of a laparoscope, a long fiber optic cable system which allows viewing of the affected area by snaking the cable from a more distant, but more easily accessible location.
There are a number of advantages to the patient with laparoscopic surgery versus the more common, open procedure. Pain and hemorrhaging are reduced due to smaller incisions and recovery times are shorter. The key element in laparoscopic surgery is the use of a laparoscope, a long fiber optic cable system which allows viewing of the affected area by snaking the cable from a more distant, but more easily accessible location.