One thing I have learned as a special education advocate is the importance of structure and consistency when it comes to the lives of those with special needs. Pearlsky and David show this need as well. Transitions are dreaded, whether it is going from one class to another, from the school year to the summer, from one grade to another, to a different school, or graduation. Change throws us off. Structure and consistency protect us.
Adults, from ‘typical’ to whack-a-doodle, also rely on consistency.
Would you be comfortable showing up for your six month dental cleaning and there is a new hygienist? How about going to get your hair done, and your hair stylist is not there and someone unknown will cut your hair? Do you prefer to go to a random mechanic every time you need one or do you go to the one you have grown to trust?
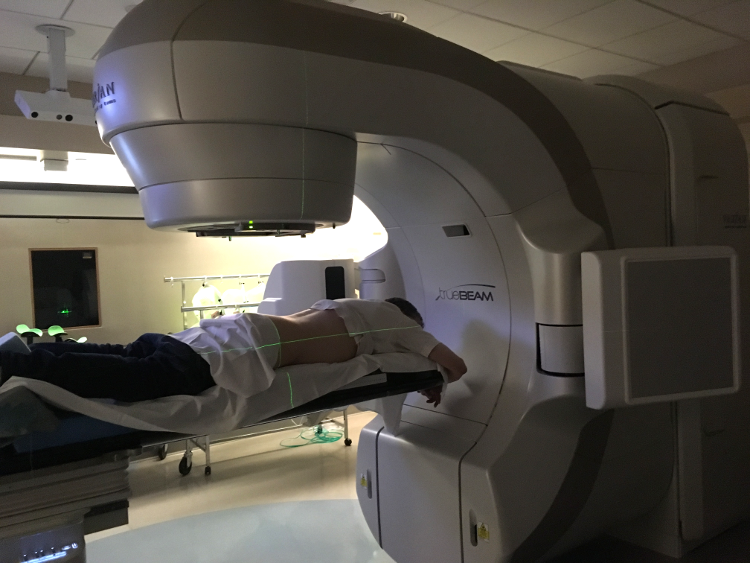
Everyday I walk up to someone sitting in front of two computer consoles who asks my name and birth date and has me confirm that the picture on one console is of me. I walk around the wall into a room with a rather large machine and that person, and one or two others, watch as I drop my pants and lie on the table. Then one of them, I never know which, lowers my skivvies, and two of them shift my position around; it’s easier to move the target (me) than the gun (giant radiation machine).
Save for Kay, they are often different, new (to me) people. Kay has been doing this for 20 years, she lies about her age (there is no way she is over her early 40’s), has a smile, confidence in her job, professional demeanor, and makes it feel ok. She has been there for 9 out of 10 of my sessions. I have no issue with whatever part of the routine she is doing. I cannot explain how unsettling it is that all the others just come and go. The same team each day would make a significant difference.
This isn’t a haircut or teeth cleaning. This is a very personal, humbling activity that includes the aiming of a gazillion megawatt beam of radiation. This concerns life and death, literally. Mine.
When it is two younger female technicians (and I do not disparage them by mentioning female because in the context, that matters) (and although I say younger, they may very well be fully trained, eminently competent, but they are not very experienced) and they have much difficulty getting me in position, it would have meant the world to me to see a familiar face … how dare Kay have a day off. I was disappointed in myself and how much it bothered me. Why did I not leave and come back when others I trusted were there? Oh yeah, can’t do that. It will just be other new people.
There are many great people in this hospital. Many who have sympathy, but few, if any, with empathy. They just don’t see what they do through the eyes of the patient. Is it really necessary to continually change the technicians? I am on the same machine, at the same time, every day.
There is a young woman who is always at the front desk in scrubs and on a computer. I have no idea what she does, who she is, etc. She is right next to the device where I scan my card when I come in. Most days she looks up and gives me a smile. In any other setting I would know her name, and schmooze for a minute or two. I don’t here, I keep to myself and just get through it. As I was leaving yesterday she looked up at me and said “have a nice weekend.” It was the first time I heard her voice, but not the first time our eyes met. I really wanted to tell her how much that meant to me, but I didn’t, I just wanted to go home. This all sucks, but without Kay or the mystery (but consistent) woman it would suck much more.
Here you can see yesterday’s scan, and yes, I shaved my beard. 😉

 Did I say “needle”? Here are two views of the same type of port, the device under my skin. And here is the catheter and needle. You can see the needle within the plastic tube/sheath. It looks rather long to me.
Did I say “needle”? Here are two views of the same type of port, the device under my skin. And here is the catheter and needle. You can see the needle within the plastic tube/sheath. It looks rather long to me.