
I showed up at 8:00 AM for my CT scan. I was told to follow the orange dots on the floor to the proper waiting room, as opposed to the green squares to the MRI waiting room. Yes, even I can do that. After a minute or two a nurse came in with my elixir to drink and asked if I wanted an IV inserted or to use my port. I forgot about my port, good idea! Close to 9:00 I was brought into the CT room, I lay on the table, and spend all of six minutes in the donut shaped machine.
Then I follow the green squares on the floor to the MRI waiting room and yes, the fun begins.
If you have not read about my first MRI experience, with the enema surprise, you really need to read that now. After my nurse practitioner heard about the experience, and then I showed her the post, she (with permission) shared it with the hospital and I got a call apologizing. Hence, make sure you remember my needing to give myself an enema on a bathroom floor, etc. before continuing to get the maximum amount of enjoyment at my continuing perverse adventure.
Again I am the only one waiting in the MRI waiting room. Within a few minutes a nurse (MRI technician?) comes out and I notice she is holding a piece of paper and … wait for it … an enema! She asks my name and birthday, confirms with the paper she is holding and tells me I need to give myself an enema. I specifically ask her where I am to do it and she points to THE SAME FUCKING BATHROOM. I then told her I gave myself one two hours ago at home and she saved the enema for another patient.
So now you should be aghast. The hospital called and apologized that they did the same exact thing twelve weeks ago hence I expected a different experience this time.
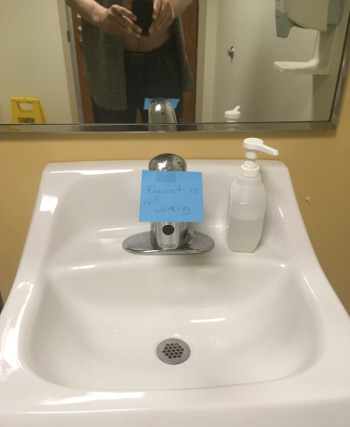
Last time I was dejected, mortified, and scared but figured it out. Unfortunately I did not get pictures of that actual bathroom and as the other post says, that is a similar bathroom. This time I was just pissed and disgusted, but I took pictures! Here is the actual bathroom where patients of this world class, big-city, ivy league teaching hospital are expected to give themselves an enema:



The astute among you will ask why there is a picture of me over the sink … no, that’s a mirror. It proves I was actually in this bathroom. But there is something the super astute of you have noticed …
But first, ENEMA 101. The result of a properly administered enema is minimally the expulsion of the contents of one’s rectum. It is typical that said expulsion is both liquid and solid. When properly done, said expulsion is done in a toilet. Note that there is a toilet in this bathroom. When said activity is occurring, solid and liquid is falling maybe six inches into water of unknown quality. Due to physics and fluid dynamics the toilet water will splash and soon it will be intermixed with said ex-contents of one’s rectum along with any bacteria, pathogens, sex toys, what-have-you. This leaves unsavory and unknown droplets of liquid on the buttocks of the enema-ee, possibly the back of the upper thighs, scrotum or vulva, and anything else placed within the porcelain ring.
Now that you have the picture (you’re welcome), you understand that the next thing the enema-ee does is reach for the super thin single-ply toilet paper to do whatever cleaning is possible. After a through study of absorption, fluid dynamics, and squeezing the Charmin, you will find that some cleaning does get accomplished and some dirtying of one’s hand(s) and fingers occurs as a result; contaminated with all manner of fecal matter and associated clean-challenged water.
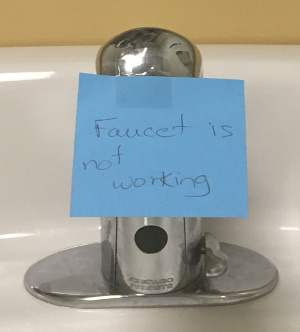
Back to the astute observers reading this. What else do you see in the photos? What’s that you say, something on the faucet?
A Post-it® note! Wonderful. Good news? The report on my CT scan? A reminder that I have rectal cancer?
But nooooooo …
So let’s review:
Three months ago I get handed an enema and shown pictures on how to give it to myself. I am told to use this very bathroom, with no place to lie down but the floor. This is so objectionable that the story of this goes from my nurse practitioner to patient relations to some administrator in radiology who reaches out to me to apologize.
Three months later, today, I am given an enema to give myself in the same bathroom. A bathroom that still has only a floor to administer said enema, but the bathroom does have a modification. A SINK THAT DOES NOT WORK. NO PLACE TO WASH ONE’S HANDS AFTERWORDS.
As I said, I gave myself an enema in the comfort of my own home earlier in the day and did not need to be demeaned by the total and complete lack of empathy on behalf of these so-called professionals. I used some soft two-ply toilet tissue followed by a brief, but effective, shower.
Readers of my blog concerning me and Pearlsky are well aware of the fact that I hate idiots. I have refrained from saying that here, and will continue to.
The MRI went fine with respect to the procedure itself. I was actually able to relax inside the machine, let’s just say better living through chemistry is more than just an expression.
We will get the results on Wednesday, in two days.

No comments yet on this ↑ post, add yours (or read theirs)